Home
Article
Archive
2000 2001
Editor:
Neil Johnston
Columnists:
Rollo
Manning
Leigh Kibby
Jon
Aldous
Roy Stevenson
Brett Clark
Ken Stafford
Pat Gallagher
Heather Pym
Simon
Rudderham
Mark
Coleman
James
Ellerson
Terry
Irvine
Roundup
Peter
Sayers
OCTOBER, Edition # 35, 2001
[Home] [About The Newsletter] [Topics Covered] [Testimonials]
Issue 19 - 17th September 2001
Depression: Part 3 Antidepressant prescribing to the elderly
* Initiating therapy for elderly patients
* Current prescribing of SSRIs to the elderly analysis of GPRN* data
* Potential interactions with SSRIsData Updates:
* Top 20 medications prescribed*The GPRN is a national Australian database of general practice data, provided by participating GPs for research purposes. The data is: anonymous patient management information electronically collected from Medical Director users who have agreed to take part longitudinal with information dating back to 1 Jan 1999 updated on a weekly basis
Health Communication Weekly covers Up-to-date information on current issues in general practice, ways to use Medical Director (MD) more effectively, information on best practice,evidence-based medicine and topics that interest you.
email us at research@hcn.com.au
Click on the Newsletter Reader's Forum link to access a forum from which you can express your comment or viewpoint on this article.
The author values your input, so please take the time to register your details, and participate in the only free debate on the future of Australian pharmacy.
Registration is free, and required once only, for permanent access.
You do not need to register if you only wish to view comments.
Computachem Editor's Note:
We are pleased to announce that we have formed an alliance with Health Communications Network (HCN), an Australian company that is heavily involved in e-health. With permission, we have extracted two items from their recent newsletter which should prove of interest to pharmacists.
Note that the second item, the top 20 prescriptions written by GP's is provided by the GPRN database noted above.Prescribing of antidepressants to the elderly
from the National Prescribing Service**This discussion of depression has been prepared for HCW by the National Prescribing Service (http://www.nps.org.au/), using GPRN data presented here.
Drug use in the elderly is often complicated by physiological changes that occur with aging, disease comorbidities, and other drugs that elderly patients are likely to take.
Renal and hepatic impairment, or reduced cardiac output may lead to increased steady state concentrations of drugs, and the aging nervous system is more sensitive to many psychotropic agents, so the risk of central adverse effects is increased.(1)
Initiating therapy for elderly patientsWhen initiating therapy with antidepressants in elderly patients, the starting dose should be at the lower end or below recommended ranges, and dose increases should be gradual as tolerated. Maintenance doses will generally be lower in older patients, but some patients will require full adult doses for a successful therapeutic effect.(1, 2)
With all antidepressants there is usually a delay of between two and four weeks before a noticeable antidepressant effect occurs, and older patients may respond even more slowly.(2)
Current prescribing of SSRIs to the elderly analysis of GPRN data
GPRN data were analysed to investigate
* rates of SSRI prescribing to the elderly and
* rates of coprescribing of :
...........warfarin
...........diureticsThe analysis was restricted to practices that had data before 1 July 99 and after 30 June 01.
This ensures that any warfarin or diuretic scripts written before Jan 2000 or after Dec 2000 that may have been concomitant with the script for SSRIs, were included.
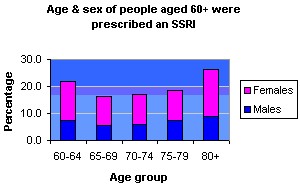
There were 923 people aged 60 or over who had a prescription for an SSRI from one of the selected practices.
Of those prescribed an SSRI, 64.6% were female (see graph).
Potential interactions with SSRIsDiuretics
Hyponatraemia is an uncommon, but increasingly recognised adverse effect associated with SSRIs, possibly caused by the syndrome of inappropriate antidiuretic hormone secretion (SIADH).
The risk of developing hyponatraemia while taking an SSRI seems to increase with age and the concomitant use of other medications that can cause hyponatraemia.
In elderly patients on SSRIs and diuretics, hyponatraemia must be suspected if confusion, lethargy or worsening of dementia occurs.(3,4)
In the analysis of GPRN data (Table 1), concomitant scripts for diuretics were held by around one fifth (21%) of patients prescribed SSRIs.Table 1: Concomitant prescriptions for SSRIs for patients >60 years
Concomitant
medicationsPatients n % SSRI and Warfarin 25 2.7% SSRI and Diuretic 192 20.8% *Percentages take into account missing values. Missing data for n=5
Warfarin
SSRIs can cause bruising and bleeding associated with platelet dysfunction.(5,6)
This effect can also increase the risk of gastrointestinal bleeding when SSRIs are given in combination with NSAIDs.(6)
In addition, some SSRIs can inhibit the metabolism of warfarin through an interaction with cytochrome P450, leading to elevations in INR.
Close monitoring of the INR is warranted if an SSRI is started, ceased or dose-adjusted when the patient is also taking warfarin.(3)
In the analysis of GPRN data (Table 1), there were a small proportion of patients (3%) who held concomitant prescriptions for SSRIs and warfarin.St Johns Wort, warfarin and SSRIs.
There is some evidence that the plant Hypericum perforatum (St Johns wort) is effective in mild to moderate depression.(7)
There are over 400 products available in Australia containing this compound, which can be purchased without a prescription.
St Johns wort may reduce the anticoagulant effect of warfarin,(8) so INR should be carefully monitored in patients who are commencing or ceasing St Johns wort.
It is also possible that combining St Johns wort with antidepressants could result in serotonin syndrome.
Five cases have been published suggestive of serotonin syndrome in elderly patients on antidepressants (sertraline or nefazodone) following the introduction of St Johns wort.(9)
Other potential interactionsSSRIs interact with many drugs as a consequence of either interactions with the cytochrome P450 enzyme system, or enhanced CNS serotonin activity.
More informationMore information about treating depression can be found on the NPS website at www.nps.org.au under Topics.
Information regarding drug interactions with SSRIs can be found in the product information for individual agents, The Australian Medicines Handbook(2) or Therapeutic Guidelines: Psychotropic(1)
References:
1. Writing Group for Therapeutic Guidelines: Psychotropic, Therapeutic Guidelines: Psychotropic. 4th edition ed. 2000, Melbourne: Therapeutic Guidelines Limited.
2. Australian Medicines Handbook. Rossi, S. ed. 2000, Adelaide: Australian Medicines Handbook Pty Ltd.
3. Drug interactions with selective serotonin reuptake inhibitors: especially with other psychotropics. Prescribe International, 2001. 10(51): p. 25-31.
4. Kirby, D. and D. Ames, Hyponatraemia and selective serotonin re-uptake inhibitors in elderly patients. International Journal of Geriatric Psychiatry, 2001. 16: p. 484-493. Adverse drugs reactions advisory committee, Bruising and bleeding with SSRIs.
5. Adverse drug reactions bulletin, 1998. 17(3): p. 10.
6. de Abajo, F.J., L.A.G. Rodriguez, and D. Montero, Association between selective serotonin reuptake inhibitors and upper gastrointestinal bleeding: population based case-control study. BMJ, 1999. 319(7217): p. 1106-1109.
7. Linde, K., et al., St John's wort for depression--an overview and meta-analysis of randomised clinical trials. BMJ, 1996. 313(7052): p. 253-258.
8. Yue, Q.-Y., C. Bergquist, and B. Gerden, Seven cases of decreased effect of warfarin during concomitant treatment with St John's wort. Lancet, 2000. 355: p. 577.
9. Lantz MS, Buchalter E, Giambanco V. St Johns wort and antidepressant drug interactions in the elderly. J Geriatr. Psychiatry Neurol 1999; 12: 7-10.
Top 20 Medications prescribed in General Practice this week
This Month Last Month This Year Generic medication Rank Percent Rank Percent Rank Percent Amoxycillin 1 4.44 1 4.0 4 2.80 Temazepam 2 3.18 3 3.0 1 3.31 Paracetamol/Codeine Phosphate 3 2.94 2 3.2 2 3.12 Paracetamol 4 2.69 4 2.5 3 2.86 Salbutamol Sulfate 5 2.20 5 2.1 6 1.83 Levonorgestrel/Ethinyloestradiol 6 2.12 6 1.9 7 1.72 Roxithromycin 7 1.96 7 1.8 12 1.31 Amoxycillin/Potassium Clavulanate 8 1.83 16 1.3 17 1.24 Doxycycline 9 1.56 9 1.5 16 1.24 Cephalexin 10 1.54 8 1.7 8 1.69 Diazepam 11 1.50 10 1.5 9 1.65 Cefaclor 12 1.38 14 1.3 21 1.04 Celecoxib 13 1.35 11 1.5 5 2.15 Simvastatin 14 1.33 17 1.2 14 1.28 Atorvastatin 15 1.32 15 1.3 15 1.27 Oxazepam 16 1.31 13 1.3 11 1.51 Omeprazole Magnesium 17 1.16 40 0.6 43 0.59 Aspirin 18 1.13 29 0.9 19 1.09 Budesonide 19 1.12 21 1.0 13 1.30 Mometasone Furoate 20 1.09 18 1.1 22 1.02
This month = four weeks ending 9 Sept 2001
Last month = four weeks ending 12 August 2001
This year = 10 September 2000 to 9 Sept 2001
Last data supplied: 9 September 2001
Data source: GPRN Health Communication Network
Editorial Review:
Geoffrey Sayer * Dr Frank Pyefinch
Contributing Authors: Fiona Horn * Leigh Hendrie * Kevin McGeechan * Geoffrey Sayer
Editor: Alice Bhasale
Health Communication Network, PO Box 67 St Leonards NSW 1590 ph 02 9906 6633 email: research@hcn.com.au.If you wish to view the full newsletter, then please follow the link
http://www.australiandoctor.com.au/healthcomms.asp
|
Previous Article |
Next Article |
Back
to Article Index
Newsletter
Reader's Forum
Article
Archive 2000
Article
Archive 2001
Home