|
PoCT was first reported in the 1980s from hospital emergency wards
in the USA where bedside testing was used to overcome poor after
hours laboratory services and the long turnaround time from the
ordering to the delivery of test results. In primary health care
settings PoCT is the on site measurement of anthropometric or body
parameters (eg body weight, height and waist circumference for obesity
), body function (eg peak flow for respiratory performance ) and
the analysis of specimens for the purposes of screening, diagnosis
or monitoring. PoCT or clinical testing in community pharmacies
both overseas and in Australia have had a chequered career due mainly
to legal and technical difficulties such as drawing specimens, quality
control and low profits (refer to C Berbatis. Essential CPE -
Clinical Testing. PSA Nov.2000 : page5).
Overseas,
these hurdles in North America and the UK have resulted in the
large groups of community pharmacies there confining their clinical
testing activities to just selling home or external testing products.
We presumed the same trend in Australia’s community pharmacies
with perhaps less than 200 or under 4% of all pharmacies nationwide
offering tests for screening and monitoring but not diagnostic
purposes. But the patterns or rates of clinical testing or any
health-related activity occurring in pharmacies anywhere in the
world are largely unknown because there are few or no published
reports with reliable national figures. Hence the potential value
of the results received from 82% of respondents in the first national
survey of health-related activities occurring in Australia’s
community pharmacies. (see editor's notes below)
Screening
for high blood pressure, cholesterol and glucose , referral of
undiagnosed clients with raised results and corrective actions
are part of a big potential role in prevention for pharmacists
or other health workers. Providing vaccines and issuing chemo-preventive
agents such as mini-dose aspirin to prevent heart disease in adults
with cardiovascular risk factors or folate for pregnant females
to prevent neural tube defects in offspring are other forms of
primary prevention practiced, to a hitherto unknown degree, by
pharmacists.
The
Guild submitted to the above Review that Australia’s 4,800
community pharmacies provide ready access to facilities, agents
and services which improve health for the public. This now appears
crucial given the high proportion of undetected risk factors in
Australia amenable to screening tests and the potential costs
savings. For example the AusDiab national survey in 2000 discovered
some 500,000 people with undiagnosed diabetes. That is, they had
been missed by the existing health system! The incidence of diabetes
is much higher than the rate of diagnosis therefore the surge
in Type 2 diabetes and costs (average $3000 per diabetic per year)
will continue unless more effective forms of screening, referral
and primary preventive interventions are introduced.
In
Curtin University’s School of Pharmacy we are analysing the
results of a survey of all community pharmacies stratified into
Pharia zone 1 ( 15% randomised) and Pharia zones 2 to 6 combined,
conducted from 12 July to September. The sample size , high rate
and representativeness of respondents allows facilities and activities
in under 1% of Australia’s pharmacies to be analysed with
95% confidence in each Pharia zone.
The
rates ( per month) and range of clinical tests ( anthropometric,
cholesterol, glucose, blood pressure, bone density, pregnancy
and other types) for screening of undiagnosed clients are being
quantified. Nationally, over 10% of pharmacies reported screening
one or more clients monthly for blood pressure and blood glucose,
or over 5% for bone density, pregnancy and anthropometric and
under 5% for blood cholesterol or other tests. Each of these national
figures must be analysed in detail and stratified. We must also
characterise ( eg by Pharia zone, shopping centre type and franchise
group) the top testing pharmacies (21 or more clients tested monthly)
.
Survey results showed almost 5% of pharmacies across Pharia zones
have community clinic services with nurses. A meta-analysis of
81 intervention studies in primary prevention found “.. teamwork
(involving nurses) and collaboration …” was the best
in improving referrals and the effectiveness of interventions
(Ann Intern Med 2002;136: 641-51). In addition to their demonstrated
effectiveness in primary prevention, nurses can overcome the problems
of specimen collection, acceptability by doctors and cost which
inhibit pharmacies currently (refer to C Berbatis. Essential
CPE - Clinical Testing. PSA Nov.2000 : page5).
We
found almost 50% of Australia’s largest pharmacies are in
franchise groups. One group of 41 pharmacies in South Australia
and Victoria engage registered nurses who circulated up to 10
times per year to conduct screening tests in consenting pharmacy
clients (undiagnosed). Based on January-June 2002 results they
screen over 12,000 cases in 12 months for hyperglycaemia, hypercholesterolaemia
and hypertension of whom approximately 15% are referred to doctors
at a cost to the group of less than $10 per referral By extrapolating
these rates to Australia’s 4800 pharmacies the national annual
referral rates total 36,000 cases for hyperglycaemia, 105,000
for hypertension and 86,000 for hypercholesterolaemia.
If
doctors examined and managed effectively to defer or prevent type
2 diabetes in just 25% of the referred hyperglycaemia patients
then gross savings exceeding $27 million for less than $0.5 million
yearly outlay by pharmacies are feasible. Australia’s incidence
(new cases) of type 2 diabetes may be cut by 10-20% per annum.
Other flow-on benefits to this pharmacy group have sustained their
continuing engagement of nurses. Analogous estimates of numbers,
savings, lowered incidence and flow-on benefits to pharmacies
may be made for the other screening tests. These promising results
need to be properly assessed and the opportunities created for
exploring these and other screening tests in this and other groups
of pharmacies.
The
recommendation by the government review combined with initial
results from respondent pharmacies in the national survey reveal
potential cost-benefits of pharmacy groups engaging nurses.
Analogous benefits are emerging from the results of the national
survey for other activities such as vaccination which have large
health and cost-benefit potential for Australia and community
pharmacies but are in danger of being lost by them.
Even at this early stage the evaluation of groups of or individual
pharmacies who currently engage nurses is warranted given the
impressive potential of and danger of losing some of the crucial
health activities they do or could perform in pharmacies.
Con Berbatis FPS(WA), MSc(Syd)
School of Pharmacy
Curtin University of Technology
Western Australia
Email : berbatis@git.com.au
October 2002
Editor's
Note:
Pharmacists should make themselves familiar
with all the work that Con Berbatis is involved with.
i2P hopes to be in a position to publish more, as the information
is made available.
Con is interested in introducing the concept that franchised market
groups need to develop their perspective in promoting and competing
with professional services. Given that 50 percent of Australian
pharmacies belong to a franchise and that 75 percent of revenue
passes through them, are they the vehicle for this type of development?
If so, what should they do?
He is also concerned with the loss of dispensing business e.g.
influenza vaccines to the over 65's and meningococcal vaccines
to the under 14's, and is exploring the thought that a select
group of pharmacies become primary health care centres and utilise
the services of nurses.
He is developing the evidence to reinforce pharmacy's professional
role in the format that governments need to base their decisions.
This is important work.
You are recommended to view the site
http://www.curtin.edu.au/curtin/dept/pharmacy/survey/index.html
and in particular, view questions 7 (on page 2) and 18 (on page
6) in the Pharmacy Survey.
Pharmacists need to be interactive to help shape this important
work, and Con Berbatis would like to hear
your views, suggestions, and further analysis of the results direct.
Please take the time to communicate to him through the active
e-mail address noted just above this paragraph.
We have also published extracts of the survey results as displayed
on the above website.
RESULTS
Response
by Pharia zone and total at 19 September 2002
Introduction
The first round of mailed questionnaires commenced on 12 July
2002, the second round began 2 August and the third and final
round from 16 August.
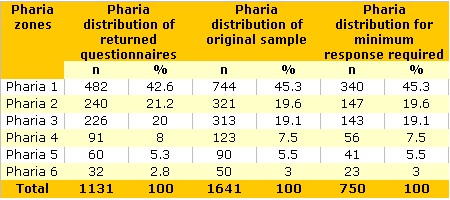
The
original sample of 1641 (middle columns) was generated by the
statistician in June 2002 and represented a 15% random sample
of all state-registered community pharmacies in Pharia zone 1
and all pharmacies in Pharia zones 2-6. These were culled and
phoned in late June by the Survey Research Centre (SRC) to obtain
the consent of participating pharmacies and the name and contact
identification of the pharmacist respondent for each consenting
pharmacy. The questionnaire was constructed and produced professionally
under Con Berbatis and Prof Bruce Sunderland of the Curtin University’s
School of Pharmacy. The SRC performed the mailed surveys, electronically
entered the data responses and obtained data from non-respondents.
The
procedures of Dillman (2000) were followed for the conduct of
the survey conducted and the construction, testing and design
of the questionnaire.
The
responses were electronically entered and the first summary was
produced in August 2002. The following summary (Table 1) compares
the number and distribution of completed questionnaires received
by 9 September 2002 and categorised by Pharia zone (left).
Results
In brief, the responses demonstrate that the level of response
obtained (left columns) far exceeded the minimum numbers required,
and the distribution accorded well with the original sample (middle).
The total response of 81% by September 9 and over 82% by 16 September
was outstanding and ranks first or in the top rank of pharmacy
or medical surveys ever conducted in the world.
The
frequency data for each section and question in were produced
by the SRC on 18th September.
Table
1. Rates and distribution of pharmacy respondents’ questionnaires
: July-September 2002 (Source: Survey Research Centre, University
of Western Australia, 18 September 2002)
Comments
These initial results will lead to cross-tabulating the data by
1 October (for initial categorising of responses by Pharia zones
and other groupings), before the final process of statistical
analysis to test relationships between features of the pharmacies
(for example the qualifications of proprietors and staff or the
range of facilities and the rate of use of these or the rate and
range of services provided). This final process will occur in
October and November 2002 for the final report to be concluded
and published by February 2003. Papers and reports have been published
in pharmacy journals (Berbatis, 2002).
References
Berbatis CG. National survey of Australia’s community pharmacies
in 2002 : rationale and methodology. J Pharm Pract Res 2002; 32:
143-6.
Dillman DA. Mail and internet surveys: the tailored design method.
Second edition. New York : John Wiley & Sons; 2000.
Source: Con Berbatis FPS(WA), MSc(Syd) School of Pharmacy Curtin
University of Technology Western Australia berbatis@git.com.au
|

.jpg)
